
Homework Answers
1)Cryptosporidium infection (cryptosporidiosis) is an illness caused by tiny, one-celled cryptosporidium parasites. When cryptosporidia (krip-toe-spoe-RID-e-uh) enter your body, they travel to your small intestine and then burrow into the walls of your intestines. Later, cryptosporidia are shed in your feces.
In most healthy people, a cryptosporidium infection produces a bout of watery diarrhea and the infection usually goes away within a week or two. If you have a compromised immune system, a cryptosporidium infection can become life-threatening without proper treatment. You can help prevent a cryptosporidium infection by practicing good hygiene and avoiding swallowing water from pools, recreational water parks, lakes and streams.
2)Cryptosporidium parvum
Cryptosporidium parvum. Cryptosporidium parvum is one of several species that cause cryptosporidiosis, a parasitic disease of the mammalian intestinal tract.
3) Causative organism is parasite.
4) Shape: Endogenous developmental stages appear as small basophilic bodies (3-6µm) attached to the luminal surface of host epithelial cells; while exogenous oocysts appear as ovoid phase-bright ovoid bodies (5-7 x 4-6µm) containing four sporozoites and an eccentric residual body.


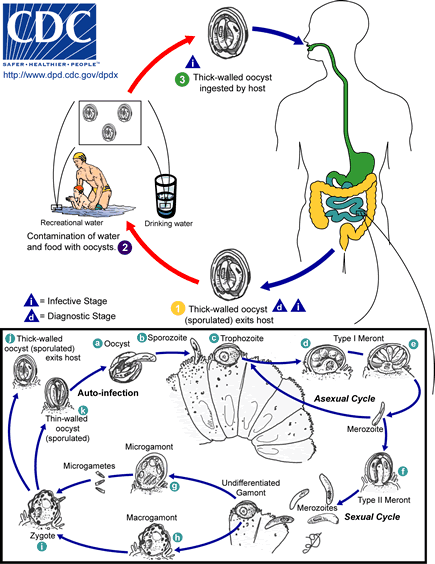
Parasite life cycle and biology
Sporulated oocysts, containing four sporozoites, are released from an infected host upon defecation. These environmentally resistant oocysts are encased in a durable oocyst wall; a complex protective barrier consisting of inner and outer oocyst walls composed of a protein-lipid-carbohydrate matrix . The infective cycle begins anew when an appropriate host ingests oocysts. The infectious dose varies depending on parasite isolate, yet as few as 10 oocysts have been reported to cause disease. Members of the genus Cryptosporidium complete all developmental stages in a single host . C. parvum oocysts excyst in the gastrointestinal tract, releasing four motile, infective sporozoites through a suture in the oocyst wall . Temperature and pH alone are sufficient to induce excystation , yet other environmental cues may include carbon dioxide, pancreatic enzymes, and bile salts . The excystation process also likely depends on parasite derived molecules including sporozoite-associated serine and cystine proteases , arginine aminopeptidase ,secretory phospholipase A2 ,and protein synthesis-associated molecules including ribosomal-associated and heat shock proteins . Through a mechanism of host cell attachment and subsequent invasion, a sporozoite is encapsulated by a parasite modified host membrane to form a parasitophorous vacuole, a structure common to apicomplexans. The parasitophorous vacuole of Cryptosporidium is unique in that it remains extracytoplasmic yet is considered intracellular as it maintains its position within the host derived parasitophorous vacuole membrane on top of epithelial cells. During internalization, a unique highly invaginated membrane, the feeder organelle, forms between the parasite and host cytoplasm. Localization studies have demonstrated that at least one of the parasite-derived ATP-binding cassette containing proteins, CpABC1, localizes to the feeder organelle and likely confers selective transport between host and parasite for nutrient uptake. The trophozoite undergoes asexual reproduction by merogony forming a Type-I meront. Cell division results in the formation of daughter cells, each surrounded by its own membrane, while still in the mother cell in a process known as endopolygeny. Under the current paradigm of C. parvum development, two developmentally distinct types of meronts are formed; Type-I and Type II .both produce merozoites, which are morphologically similar to sporozoites.
5)
The mechanism by which Cryptosporidium causes diarrhea includes a combination of increased intestinal permeability, chloride secretion, and malabsorption, which are all thought to be caused by the host response to infection. In immunocompetent persons, the infection is usually limited to the small intestine.
As few as 2 to 10 oocysts can initiate an infection.The parasite is located in the brush border of the epithelial cells of the small intestine. They are mainly located in the jejunum. When the sporozoites attach the epithelial cells’ membrane envelops them. Thus, they are “intracellular but extracytoplasmic”.The parasite can cause damage to the microvilli where it attaches.The infected human excretes the most oocysts during the first week. Oocysts can be excreted for weeks after the diarrhea subsides from infections by C. parvum or C. hominis;however, immunocompetent individuals with C. muris infections have been observed excreting oocysts for seven months.
6)
The first signs and symptoms of cryptosporidium infection usually appear within a week after infection and may include:
- Watery diarrhea
- Dehydration
- Lack of appetite
- Weight loss
- Stomach cramps or pain
- Fever
- Nausea
- Vomiting
Worsening of symptoms may be characterised by severe signs of dehydration such as sunken eye balls, decreased skin turgor and hypovolemic shock.
7) Mode of transmission is mainly feco- oral route
Cryptosporidium infection begins when you ingest the one-celled cryptosporidium parasite. Some strains of cryptosporidium may cause more serious disease.
These parasites then travel to your intestinal tract, where they settle into the walls of your intestines. Eventually, more cells are produced and shed in massive quantities into your feces, where they are highly contagious.
You can become infected with cryptosporidia by touching anything that has come in contact with contaminated feces. Methods of infection include:
- Drinking contaminated water that contains cryptosporidium parasites
- Swimming in contaminated water that contains cryptosporidium parasites and accidentally swallowing some of it
- Eating uncooked, contaminated food that contains cryptosporidia
- Touching your hand to your mouth if your hand has been in contact with a contaminated surface or object
- Having close contact with other infected people or animals — especially their feces — which can allow the parasite to be transmitted from your hands to your mouth.
8)The simplest way to diagnose cryptosporidium infection is a method called an acid-staining test, which identifies cryptosporidium under a microscope. To obtain cells for the analysis, your doctor might ask for a stool sample, or in more extreme cases, take a tissue sample (biopsy) from your intestine for the test.
- Stool culture. Your doctor might also order a standard stool culture. Although this test cannot detect the presence of cryptosporidium, it may help rule out other bacterial pathogens.
- Other tests. Once it's clear that your infection is caused by cryptosporidium parasites, you may need further testing to check for development of serious complications. For example, checking liver and gallbladder function may determine whether the infection has spread. If you have both AIDS and cryptosporidiosis, a T-cell count — which measures the level of a certain white blood cell that's part of your immune system — can help predict the duration of the cryptosporidiosis. A T-cell count under 100 cells per microliter means you're more likely to have complications.
9)
- Anti-parasitic drugs. Medications, such as nitazoxanide (Alinia), can help alleviate diarrhea by attacking the metabolic processes of the cryptosporidium organisms. Azithromycin (Zithromax) may be given along with one of these medications in people with compromised immune systems.
- Anti-motility agents. These medications slow down the movements of your intestines and increase fluid absorption to relieve diarrhea and restore normal stools. Anti-motility drugs include loperamide and its derivatives (Imodium A-D, others). Talk with your doctor before taking any of these medications.
- Fluid replacement. You'll need either oral or intravenous replacement of fluids and electrolytes — minerals, such as sodium, potassium and calcium, that maintain the balance of fluids in your body — lost to persistent diarrhea. These precautions will help keep your body hydrated and functioning properly.
- Antiretroviral therapies. If you have HIV/AIDS, highly active antiretroviral therapy (HAART) can reduce the viral load in your body and boost your immune response. Restoring your immune system to a certain level may completely resolve symptoms of cryptosporidiosis.
10) Risk for exposure should be determined which is:
People who are at increased risk of developing cryptosporidiosis include:
- Those who are exposed to contaminated water.
- Children, particularly those wearing diapers, who attend child care centers.
- Parents of infected children.
- Child care workers.
- Animal handlers.
- Those who engage in oral-to-anal sexual activity.
11) Cryptosporidiosis is a nationally notifiable disease in United kingdom.
12)Prevalence rates reported in large-scale surveys of fecal oocyst excretion generally range from 1-3% in developed countries in Europe and North America. Children, especially those younger than 2 years, appear to have a higher prevalence of infection than do adults.
Cryptosporidiosis is a notifiable disease at the European Union level, and surveillance data are collected through the European Basic Surveillance Network. The crude incidence rate was similar to that in the United States, although considerable differences in the rates of cryptosporidiosis between countries were observed.A pronounced seasonal peak was observed in the autumn season, with 59% of cases reported between August and November. However, Ireland and Spain experienced a peak in spring and summer, respectively. Routine cryptosporidiosis surveillance in northwest England over 17 years revealed that cases predominantly occurred in spring and autumn. There, most infections are caused by C hominis, while C parvum is associated with rural areas and animal contact.
14) References
-
White AC Jr. Cryptosporidiosis (Cryptosporidium species). Bennett JE, Dolin R, Blaser MK, eds. Principles and Practice of Infectious Diseases. 8th ed. Philadelphia, Pa: Elsevier Churchill Livingstone; 2015. Chapter 284, pages 3173-83.
-
Checkley W, White AC Jr, Jaganath D, Arrowood MJ, Chalmers RM, Chen XM, et al. A review of the global burden, novel diagnostics, therapeutics, and vaccine targets for cryptosporidium. Lancet Infect Dis. 2015 Jan. 15 (1):85-94. [Medline].
-
Bouzid M, Hunter PR, Chalmers RM, Tyler KM. Cryptosporidium pathogenicity and virulence. Clin Microbiol Rev. 2013 Jan. 26(1):115-34. [Medline]. [Full Text].
-
Yoder JS, Beach MJ. Cryptosporidium surveillance and risk factors in the United States. Exp Parasitol. 2010 Jan. 124(1):31-9. [Medline].
-
Painter JE, Hlavsa MC, Collier SA, Xiao L, Yoder JS, Centers for Disease Control and Prevention. Cryptosporidiosis surveillance -- United States, 2011-2012. MMWR Suppl. 2015 May 1. 64 (3):1-14. [Medline].
-
Chalmers RM, Smith R, Elwin K, Clifton-Hadley FA, Giles M. Epidemiology of anthroponotic and zoonotic human cryptosporidiosis in England and Wales, 2004-2006. Epidemiol Infect. 2011 May. 139(5):700-12. [Medline].
-
Scallan E, Hoekstra RM, Angulo FJ, Tauxe RV, Widdowson MA, Roy SL, et al. Foodborne illness acquired in the United States--major pathogens. Emerg Infect Dis. 2011 Jan. 17(1):7-15. [Medline]. [Full Text].
-
Mac Kenzie WR, Hoxie NJ, Proctor ME, Gradus MS, Blair KA, Peterson DE, et al. A massive outbreak in Milwaukee of cryptosporidium infection transmitted through the public water supply. N Engl J Med. 1994 Jul 21. 331(3):161-7. [Medline].
-
Chalmers RM. Waterborne outbreaks of cryptosporidiosis. Ann Ist Super Sanita. 2012. 48 (4):429-46. [Medline].
-
Semenza JC, Nichols G. Cryptosporidiosis surveillance and water-borne outbreaks in Europe. Euro Surveill. 2007 May 1. 12(5):E13-4. [Medline].
-
Cooper DL, Verlander NQ, Smith GE, Charlett A, Gerard E, Willocks L, et al. Can syndromic surveillance data detect local outbreaks of communicable disease? A model using a historical cryptosporidiosis outbreak. Epidemiol Infect. 2006 Feb. 134(1):13-20. [Medline]. [Full Text].
-
Fournet N, Deege MP, Urbanus AT, Nichols G, Rosner BM, Chalmers RM, et al. Simultaneous increase of Cryptosporidium infections in the Netherlands, the United Kingdom and Germany in late summer season, 2012. Euro Surveill. 2013 Jan 10. 18(2):[Medline].
-
Ajjampur SS, Rajendran P, Ramani S, Banerjee I, Monica B, Sankaran P, et al. Closing the diarrhoea diagnostic gap in Indian children by the application of molecular techniques. J Med Microbiol. 2008 Nov. 57:1364-8. [Medline].
-
Shirley DA, Moonah SN, Kotloff KL. Burden of disease from cryptosporidiosis. Curr Opin Infect Dis. 2012 Oct. 25(5):555-63. [Medline].
-
Nair P, Mohamed JA, DuPont HL, Figueroa JF, Carlin LG, Jiang ZD, et al. Epidemiology of cryptosporidiosis in North American travelers to Mexico. Am J Trop Med Hyg. 2008 Aug. 79(2):210-4. [Medline]. [Full Text].
-
O'connor RM, Shaffie R, Kang G, Ward HD. Cryptosporidiosis in patients with HIV/AIDS. AIDS. 2011 Mar 13. 25(5):549-60. [Medline].
-
Wang L, Zhang H, Zhao X, Zhang L, Zhang G, Guo M, et al. Zoonotic Cryptosporidium species and Enterocytozoon bieneusi genotypes in HIV-positive patients on antiretroviral therapy. J Clin Microbiol. 2013 Feb. 51(2):557-63. [Medline]. [Full Text].
-
Wumba R, Longo-Mbenza B, Mandina M, Odio WT, Biligui S, Sala J, et al. Intestinal parasites infections in hospitalized AIDS patients in Kinshasa, Democratic Republic of Congo. Parasite. 2010 Dec. 17(4):321-8. [Medline].
-
Mondal D, Haque R, Sack RB, Kirkpatrick BD, Petri WA Jr. Attribution of malnutrition to cause-specific diarrheal illness: evidence from a prospective study of preschool children in Mirpur, Dhaka, Bangladesh. Am J Trop Med Hyg. 2009 May. 80(5):824-6. [Medline]. [Full Text].
-
Guerrant DI, Moore SR, Lima AA, Patrick PD, Schorling JB, Guerrant RL. Association of early childhood diarrhea and cryptosporidiosis with impaired physical fitness and cognitive function four-seven years later in a poor urban community in northeast Brazil. Am J Trop Med Hyg. 1999 Nov. 61(5):707-13. [Medline].
-
Amadi B, Mwiya M, Musuku J, Watuka A, Sianongo S, Ayoub A, et al. Effect of nitazoxanide on morbidity and mortality in Zambian children with cryptosporidiosis: a randomised controlled trial. Lancet. 2002 Nov 2. 360(9343):1375-80. [Medline].
-
Vakil NB, Schwartz SM, Buggy BP, Brummitt CF, Kherellah M, Letzer DM, et al. Biliary cryptosporidiosis in HIV-infected people after the waterborne outbreak of cryptosporidiosis in Milwaukee. N Engl J Med. 1996 Jan 4. 334(1):19-23. [Medline].
-
Chalmers RM, Campbell BM, Crouch N, Charlett A, Davies AP. Comparison of diagnostic sensitivity and specificity of seven Cryptosporidium assays used in the UK. J Med Microbiol. 2011 Nov. 60:1598-604. [Medline].
-
Committee on Infectious Diseases, American Academy of Pediatrics. Cryptosporidiosis. Kimberlin DW, Brady MT, Jackson MA, Long Ss, eds. Red Book. 30th ed. Elk Grove Village, Ill: American Academy of Pediatrics; 2015. 312-18.
-
Hunter PR, Nichols G. Epidemiology and clinical features of Cryptosporidium infection in immunocompromised patients. Clin Microbiol Rev. 2002 Jan. 15(1):145-54. [Medline]. [Full Text].
-
Rossignol JF, Kabil SM, el-Gohary Y, Younis AM. Effect of nitazoxanide in diarrhea and enteritis caused by Cryptosporidium species. Clin Gastroenterol Hepatol. 2006 Mar. 4(3):320-4. [Medline].
-
Rossignol JF, Ayoub A, Ayers MS. Treatment of diarrhea caused by Cryptosporidium parvum: a prospective randomized, double-blind, placebo-controlled study of Nitazoxanide. J Infect Dis. 2001 Jul 1. 184(1):103-6. [Medline].
-
Cabada MM, White AC Jr. Treatment of cryptosporidiosis: do we know what we think we know?. Curr Opin Infect Dis. 2010 Oct. 23(5):494-9. [Medline].
-
Pantenburg B, White AC Jr. Nitazoxanide. In: Grayson ML, ed. Kucer’s The Use of Antibiotics. 6th ed. London, United Kingdom: Hodder Arnold; 2010:2132-9.
-
Smith NH, Cron S, Valdez LM, Chappell CL, White AC Jr. Combination drug therapy for cryptosporidiosis in AIDS. J Infect Dis. 1998 Sep. 178(3):900-3. [Medline].
-
Masur H, Brooks JT, Benson CA, Holmes KK, Pau AK, Kaplan JE, et al. Prevention and treatment of opportunistic infections in HIV-infected adults and adolescents: Updated Guidelines from the Centers for Disease Control and Prevention, National Institutes of Health, and HIV Medicine Association of the Infectious Diseases Society of America. Clin Infect Dis. 2014 May. 58 (9):1308-11. [Medline]. [Full Text].
-
Hicks P, Zwiener RJ, Squires J, Savell V. Azithromycin therapy for Cryptosporidium parvum infection in four children infected with human immunodeficiency virus. J Pediatr. 1996 Aug. 129(2):297-300. [Medline].
-
Centers for Disease Control and Prevention. Parasites – Cryptosporidium (also knows as "Crypto"). Cdc.com. Available at http://www.cdc.gov/parasites/crypto/. Accessed: April 9, 2013.
-
Amadi B, Mwiya M, Sianongo S, Payne L, Watuka A, Katubulushi M, et al. High dose prolonged treatment with nitazoxanide is not effective for cryptosporidiosis in HIV positive Zambian children: a randomised controlled trial. BMC Infect Dis. 2009 Dec 2. 9:195. [Medline]. [Full Text].
-
Cama VA, Bern C, Roberts J, Cabrera L, Sterling CR, Ortega Y, et al. Cryptosporidium species and subtypes and clinical manifestations in children, Peru. Emerg Infect Dis. 2008 Oct. 14(10):1567-74. [Medline]. [Full Text].
Add Answer to:
Case Report #5 On July 4, 2007, Florida's Central District Health Department (CDHD) received a complaint...
Case Report #5 On July 4, 2007, Florida's Central District Health Department (CDHD) received a complaint...
 Case Report #5 On July 4, 2007, Florida's Central District Health Department (CDHD) received a complaint of several ill persons with watery diarrhea after attendance at a municipal splash park on June 26. Water samples collected from splash features and an adjacent drinking fountain tested positive. The report by Florida Department of Health summarized the investigation of the outbreak and highlights the importance of splash park design, operation, access to hygiene facilities, and public education in prevention of waterbome parasites...
Case Report #5 On July 4, 2007, Florida's Central District Health Department (CDHD) received a complaint of several ill persons with watery diarrhea after attendance at a municipal splash park on June 26. Water samples collected from splash features and an adjacent drinking fountain tested positive. The report by Florida Department of Health summarized the investigation of the outbreak and highlights the importance of splash park design, operation, access to hygiene facilities, and public education in prevention of waterbome parasites...
Case Report # 5 On July 4, 2007, Florida's Central District Health Department (CDHD) received a...
 Case Report # 5 On July 4, 2007, Florida's Central District Health Department (CDHD) received a complaint of several ill persons with watery diarrhea after attendance at a municipal splash park on June 26. Water samples collected from splash features and an adjacent drinking fountain tested positive. The report by Florida Department of Health summarized the investigation of the outbreak and highlights the importance of splash park design, operation, access to hygiene facilities, and public education in prevention of waterborne...
Case Report # 5 On July 4, 2007, Florida's Central District Health Department (CDHD) received a complaint of several ill persons with watery diarrhea after attendance at a municipal splash park on June 26. Water samples collected from splash features and an adjacent drinking fountain tested positive. The report by Florida Department of Health summarized the investigation of the outbreak and highlights the importance of splash park design, operation, access to hygiene facilities, and public education in prevention of waterborne...
EXOTIC PARASITE SICKENS CANADIAN BUSINESSMEN Public health officials today confirmed that three Canadian business men, two...
 EXOTIC PARASITE SICKENS CANADIAN BUSINESSMEN Public health officials today confirmed that three Canadian business men, two from Toronto and one from Ottawa, were diagnosed cyclosporiasis, a parasitic disease seen only in tropical countries and overseas travelers. The three men, who had recently traveled to the United States, became seriously il with diarrhea over the weekend (May 16-18). One of the men was hospitalized at Princess Margaret Hospital when he collapsed due to severe dehydration. Dr. Richard Schabas, Ontario's Chief Medical...
EXOTIC PARASITE SICKENS CANADIAN BUSINESSMEN Public health officials today confirmed that three Canadian business men, two from Toronto and one from Ottawa, were diagnosed cyclosporiasis, a parasitic disease seen only in tropical countries and overseas travelers. The three men, who had recently traveled to the United States, became seriously il with diarrhea over the weekend (May 16-18). One of the men was hospitalized at Princess Margaret Hospital when he collapsed due to severe dehydration. Dr. Richard Schabas, Ontario's Chief Medical...
The following information has just come into a State Department of Health. Clinical laboratories reported a...
The following information has just come into a State Department of Health. Clinical laboratories reported a significant increase in demand for the media to perform routine stool cultures, resulting in requests to other labs and the State Department of Health for additional supplies. Pharmacists are reporting difficulty keeping over the counter and prescription antidiarrheal medication in stock. The local water authority was deluged by complaints from customers about increased water turbidity and water that tasted and smelled unpleasant. Additionally, school...
EXOTIC PARASITE SICKENS CANADIAN BUSINESSMEN Public health officials today confirmed that three Canadian business men, two...
 EXOTIC PARASITE SICKENS CANADIAN BUSINESSMEN Public health officials today confirmed that three Canadian business men, two from Toronto and one from Ottawa, were diagnosed sxclosporiasis, a parastic disease seen only in tropical countries and overseas travelers. The three men, who had recently traveled to the United States, became seriouslyill with diarrhea over the weekend (May 16-18). One of the men was hospitalized at Princess Margaret Hospital when he collapsed due to severe dehydration. Dr. Richard Schabas, Ontario's Chief Medical Officer,...
EXOTIC PARASITE SICKENS CANADIAN BUSINESSMEN Public health officials today confirmed that three Canadian business men, two from Toronto and one from Ottawa, were diagnosed sxclosporiasis, a parastic disease seen only in tropical countries and overseas travelers. The three men, who had recently traveled to the United States, became seriouslyill with diarrhea over the weekend (May 16-18). One of the men was hospitalized at Princess Margaret Hospital when he collapsed due to severe dehydration. Dr. Richard Schabas, Ontario's Chief Medical Officer,...
can't save changes to this file. Outbreak Investigation (Updated) You have been called in by Mammoth Lake's...
 can't save changes to this file. Outbreak Investigation (Updated) You have been called in by Mammoth Lake's health department to investigate a local summer camp called Camp Mammoth Lake. Some of the campers have become ill with gastrointestinal (GI) symptoms, including diarrhea, abdominal cramps, muscle pain, fever, nausea, and/or vomiting. The counselors noted that the first child become ill on July 1. Unfortunately, those with signs and symptoms were sent home from the camp and stool samples were not obtained...
can't save changes to this file. Outbreak Investigation (Updated) You have been called in by Mammoth Lake's health department to investigate a local summer camp called Camp Mammoth Lake. Some of the campers have become ill with gastrointestinal (GI) symptoms, including diarrhea, abdominal cramps, muscle pain, fever, nausea, and/or vomiting. The counselors noted that the first child become ill on July 1. Unfortunately, those with signs and symptoms were sent home from the camp and stool samples were not obtained...
PART 1 Case Information: You are a public health officer on a population Pacific island. You...
 PART 1 Case Information: You are a public health officer on a population Pacific island. You receive a call on October 5 from an occupational physician who describes an outbreak of unusual illness that began during the last week of September among workers at a printing factory. The physician tells you that a number of workers became ill within a 2 to 3-day period. Their symptoms included double vision, drooping eyelids, muscle weakness, and progressive respiratory weakness. Two workers have...
PART 1 Case Information: You are a public health officer on a population Pacific island. You receive a call on October 5 from an occupational physician who describes an outbreak of unusual illness that began during the last week of September among workers at a printing factory. The physician tells you that a number of workers became ill within a 2 to 3-day period. Their symptoms included double vision, drooping eyelids, muscle weakness, and progressive respiratory weakness. Two workers have...
354 EAK IN THE CAPSTONE CASE A: HEPATITIS A OUTBREAK MIDWEST By Catherine Dentinger and Steven...
 354 EAK IN THE CAPSTONE CASE A: HEPATITIS A OUTBREAK MIDWEST By Catherine Dentinger and Steven T. Fleming cases of hepatitis JL (1990 population ne first 30 weeks 5) was reported 5). In County anti-HAV) were inued from previous CITY ONE OUTBREA Case Definition: Apr with a discrete onset ber 3, 1998, who wa link to a laboratory October 15 and Dece Case Finding: The N county health depa requested counties state. County R He: ing all emergency county and...
354 EAK IN THE CAPSTONE CASE A: HEPATITIS A OUTBREAK MIDWEST By Catherine Dentinger and Steven T. Fleming cases of hepatitis JL (1990 population ne first 30 weeks 5) was reported 5). In County anti-HAV) were inued from previous CITY ONE OUTBREA Case Definition: Apr with a discrete onset ber 3, 1998, who wa link to a laboratory October 15 and Dece Case Finding: The N county health depa requested counties state. County R He: ing all emergency county and...
In one recent 2-week summer period, the Fairview County Health Department (FCHD) received 4 reports from...
In one recent 2-week summer period, the Fairview County Health Department (FCHD) received 4 reports from local physicians of E. coli infection (a mandatory reportable disease) among child patients. Fearing a more extensive outbreak, the FCHD Director immediately started active case-finding procedures, because the peak summer tourist season was still ahead. By the fifth week, the FCHD had identified five more reports of E. coli infection in children - all of whom had visited the Daisy Farm Petting Zoo. The...
Case 1 A 19-year-old male college student presents to the student health department with abdominal pain,...
Case 1 A 19-year-old male college student presents to the student health department with abdominal pain, diarrhea, and fever. He say that his symptoms started 1 day ago. He has had 10 stools in the past day and has noted blood mixed in with the stool on several occasions. He usually eats at home but reports having eaten chicken in the college cafeteria days ago. He has no history of gastrointestinal (GI) disease. On examination he has a temperature of...
 Case Report #5 On July 4, 2007, Florida's Central District Health Department (CDHD) received a complaint of several ill persons with watery diarrhea after attendance at a municipal splash park on June 26. Water samples collected from splash features and an adjacent drinking fountain tested positive. The report by Florida Department of Health summarized the investigation of the outbreak and highlights the importance of splash park design, operation, access to hygiene facilities, and public education in prevention of waterbome parasites...
Case Report #5 On July 4, 2007, Florida's Central District Health Department (CDHD) received a complaint of several ill persons with watery diarrhea after attendance at a municipal splash park on June 26. Water samples collected from splash features and an adjacent drinking fountain tested positive. The report by Florida Department of Health summarized the investigation of the outbreak and highlights the importance of splash park design, operation, access to hygiene facilities, and public education in prevention of waterbome parasites...
 Case Report # 5 On July 4, 2007, Florida's Central District Health Department (CDHD) received a complaint of several ill persons with watery diarrhea after attendance at a municipal splash park on June 26. Water samples collected from splash features and an adjacent drinking fountain tested positive. The report by Florida Department of Health summarized the investigation of the outbreak and highlights the importance of splash park design, operation, access to hygiene facilities, and public education in prevention of waterborne...
Case Report # 5 On July 4, 2007, Florida's Central District Health Department (CDHD) received a complaint of several ill persons with watery diarrhea after attendance at a municipal splash park on June 26. Water samples collected from splash features and an adjacent drinking fountain tested positive. The report by Florida Department of Health summarized the investigation of the outbreak and highlights the importance of splash park design, operation, access to hygiene facilities, and public education in prevention of waterborne...
 EXOTIC PARASITE SICKENS CANADIAN BUSINESSMEN Public health officials today confirmed that three Canadian business men, two from Toronto and one from Ottawa, were diagnosed cyclosporiasis, a parasitic disease seen only in tropical countries and overseas travelers. The three men, who had recently traveled to the United States, became seriously il with diarrhea over the weekend (May 16-18). One of the men was hospitalized at Princess Margaret Hospital when he collapsed due to severe dehydration. Dr. Richard Schabas, Ontario's Chief Medical...
EXOTIC PARASITE SICKENS CANADIAN BUSINESSMEN Public health officials today confirmed that three Canadian business men, two from Toronto and one from Ottawa, were diagnosed cyclosporiasis, a parasitic disease seen only in tropical countries and overseas travelers. The three men, who had recently traveled to the United States, became seriously il with diarrhea over the weekend (May 16-18). One of the men was hospitalized at Princess Margaret Hospital when he collapsed due to severe dehydration. Dr. Richard Schabas, Ontario's Chief Medical...
 EXOTIC PARASITE SICKENS CANADIAN BUSINESSMEN Public health officials today confirmed that three Canadian business men, two from Toronto and one from Ottawa, were diagnosed sxclosporiasis, a parastic disease seen only in tropical countries and overseas travelers. The three men, who had recently traveled to the United States, became seriouslyill with diarrhea over the weekend (May 16-18). One of the men was hospitalized at Princess Margaret Hospital when he collapsed due to severe dehydration. Dr. Richard Schabas, Ontario's Chief Medical Officer,...
EXOTIC PARASITE SICKENS CANADIAN BUSINESSMEN Public health officials today confirmed that three Canadian business men, two from Toronto and one from Ottawa, were diagnosed sxclosporiasis, a parastic disease seen only in tropical countries and overseas travelers. The three men, who had recently traveled to the United States, became seriouslyill with diarrhea over the weekend (May 16-18). One of the men was hospitalized at Princess Margaret Hospital when he collapsed due to severe dehydration. Dr. Richard Schabas, Ontario's Chief Medical Officer,...
 can't save changes to this file. Outbreak Investigation (Updated) You have been called in by Mammoth Lake's health department to investigate a local summer camp called Camp Mammoth Lake. Some of the campers have become ill with gastrointestinal (GI) symptoms, including diarrhea, abdominal cramps, muscle pain, fever, nausea, and/or vomiting. The counselors noted that the first child become ill on July 1. Unfortunately, those with signs and symptoms were sent home from the camp and stool samples were not obtained...
can't save changes to this file. Outbreak Investigation (Updated) You have been called in by Mammoth Lake's health department to investigate a local summer camp called Camp Mammoth Lake. Some of the campers have become ill with gastrointestinal (GI) symptoms, including diarrhea, abdominal cramps, muscle pain, fever, nausea, and/or vomiting. The counselors noted that the first child become ill on July 1. Unfortunately, those with signs and symptoms were sent home from the camp and stool samples were not obtained...
 PART 1 Case Information: You are a public health officer on a population Pacific island. You receive a call on October 5 from an occupational physician who describes an outbreak of unusual illness that began during the last week of September among workers at a printing factory. The physician tells you that a number of workers became ill within a 2 to 3-day period. Their symptoms included double vision, drooping eyelids, muscle weakness, and progressive respiratory weakness. Two workers have...
PART 1 Case Information: You are a public health officer on a population Pacific island. You receive a call on October 5 from an occupational physician who describes an outbreak of unusual illness that began during the last week of September among workers at a printing factory. The physician tells you that a number of workers became ill within a 2 to 3-day period. Their symptoms included double vision, drooping eyelids, muscle weakness, and progressive respiratory weakness. Two workers have...
 354 EAK IN THE CAPSTONE CASE A: HEPATITIS A OUTBREAK MIDWEST By Catherine Dentinger and Steven T. Fleming cases of hepatitis JL (1990 population ne first 30 weeks 5) was reported 5). In County anti-HAV) were inued from previous CITY ONE OUTBREA Case Definition: Apr with a discrete onset ber 3, 1998, who wa link to a laboratory October 15 and Dece Case Finding: The N county health depa requested counties state. County R He: ing all emergency county and...
354 EAK IN THE CAPSTONE CASE A: HEPATITIS A OUTBREAK MIDWEST By Catherine Dentinger and Steven T. Fleming cases of hepatitis JL (1990 population ne first 30 weeks 5) was reported 5). In County anti-HAV) were inued from previous CITY ONE OUTBREA Case Definition: Apr with a discrete onset ber 3, 1998, who wa link to a laboratory October 15 and Dece Case Finding: The N county health depa requested counties state. County R He: ing all emergency county and...
Most questions answered within 3 hours.
-
A 1400Kg sports car accelerates from rest to 90km/h in 7.0s.
What is the average power...
asked 10 minutes ago -
For the following reaction, 0.128 moles of
potassium hydrogen sulfateare mixed with
0.504 moles of potassium...
asked 3 hours ago -
1. What is the present value of $400, three years in the future
if the interest...
asked 4 hours ago -
The labor force minus the number of employed equals the number
of unemployed.
a. True
b....
asked 6 hours ago -
Determine the mass in units of grams [g] of 0.49 moles [mol]
of a new fictitious...
asked 6 hours ago -
A horizontal mass of M=5kg is on a spring and stretched to
x=0.5m when released from...
asked 8 hours ago -
26 of 50
"I have worked at the Arizona Humane Society for ten years, and
have...
asked 8 hours ago -
Compare and contrast zero based budgeting and incremental (or
base year) budgeting.
asked 8 hours ago -
4 pts 10. Which of the following hypothesis would be MOST
difficult to test experimentally? Group...
asked 8 hours ago -
A business owner makes 1,000 items a day. Each day he or she
contributes eight hours...
asked 8 hours ago -
A
circular loop in the plane of a paper lies inca0.65 T magnetic
field pointing into...
asked 8 hours ago -
A business owner is trying to decide whether to buy, rent, or
lease office space and...
asked 8 hours ago