Ch 10.2
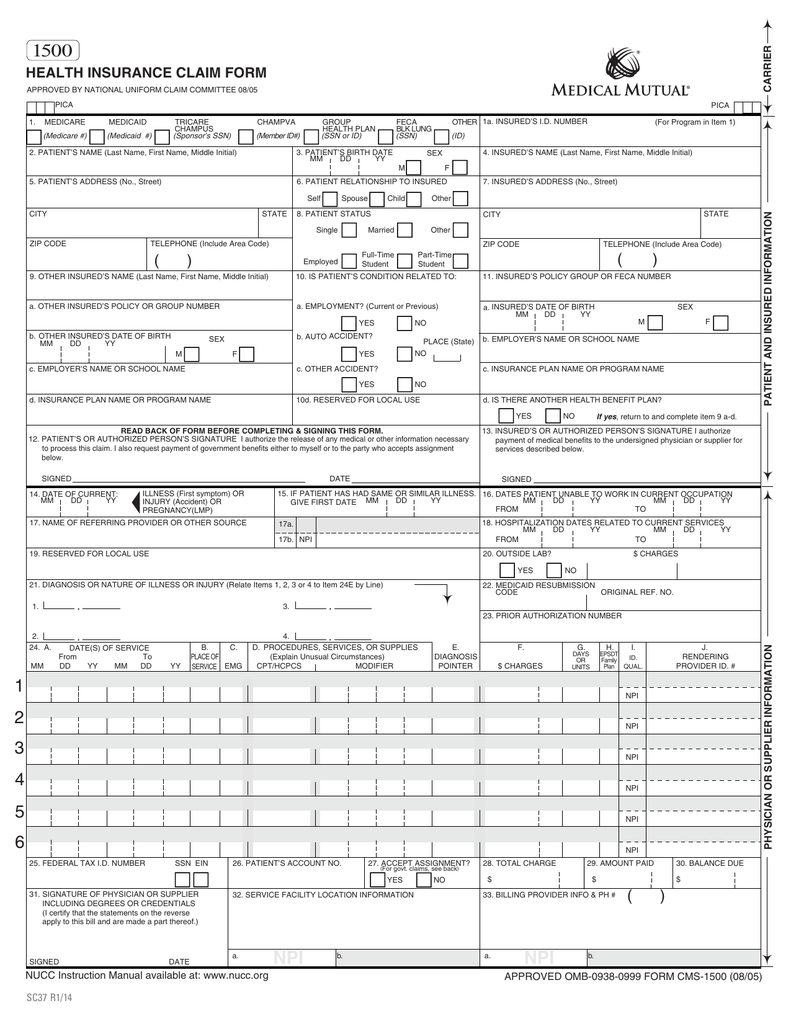
The objective of these exercises is to correctly complete Medicaid claims, applying what you have learned in the chapter. Following the information about the provider for the cases are two sections. The first section contains information about the patient, the insurance coverage, and the current medical condition. The second section is an encounter form for Valley Associates, PC.
Billing Provider Information
Name: Valley Associates, PC
Address: 1400 West Center Street
Toledo, OH
43601-0213
Telephone: 555-967-0303
Employer ID Number: 16-1234567
NPI: 1476543215
Rendering Provider Information
Name: David Rosenberg, MD
NPI: 1288560027
Assignment: Accepts
Signature: On File (01/01/2029)
nformation About the Patient:
Name: Scott Yeager
Sex: M
Birth Date: 11/17/1974
Marital Status: Single
Address: 301 Maple Ave.
Sandusky, OH
44870-4567
Telephone: 555-626-7268
Employer: Unemployed
Race: White
Ethnicity: Not Hispanic or Latino
Preferred Language: English
Insured: Self
Health Plan: Medicaid
Insurance ID Number: 139629748MC
Policy Number: 75324
Group Number: N/A for Medicaid Plans
Copayment/Deductible Amt.: $15 copay
Assignment of Benefits: Y
Signature on File: 10/01/2029
Condition Unrelated to Employment, Auto Accident, or Other Accident

Homework Answers
Request Answer!
10 have requested this problem solution
The more requests, the faster the answer.
Ch 10.1
 The objective of these exercises is to correctly complete Medicaid claims, applying what you have learned in the chapter. Following the information about the provider for the cases are two sections. The first section contains information about the patient, the insurance coverage, and the current medical condition. The second section is an encounter form for Valley Associates, PC. Billing Provider Information Name: Valley Associates, PCAddress: 1400 West Center Street Toledo, OH 43601-0213Telephone: 555-967-0303Employer ID Number: 16-1234567NPI: 1476543215 Rendering Provider Information Name: David Rosenberg, MDNPI: 1288560027Assignment: AcceptsSignature: On File (01/01/2029)
The objective of these exercises is to correctly complete Medicaid claims, applying what you have learned in the chapter. Following the information about the provider for the cases are two sections. The first section contains information about the patient, the insurance coverage, and the current medical condition. The second section is an encounter form for Valley Associates, PC. Billing Provider Information Name: Valley Associates, PCAddress: 1400 West Center Street Toledo, OH 43601-0213Telephone: 555-967-0303Employer ID Number: 16-1234567NPI: 1476543215 Rendering Provider Information Name: David Rosenberg, MDNPI: 1288560027Assignment: AcceptsSignature: On File (01/01/2029)
Ch 15 Case Studies #3
 Prepare the claim for this case by completing the appropriate fields in the CMS-1500 form provided. Accuracy is important.Billing Provider: Valley Associates, PCNPI: 1476543215Employer ID Number: 16-1234567Address: 1400 West Center Street, Toledo, OH 43601-0213Telephone: 555-967-0303Rendering Provider: Christopher M. Connolly, MDNPI: 8877365552Assignment: AcceptsSignature: On File (01/01/2029)
Prepare the claim for this case by completing the appropriate fields in the CMS-1500 form provided. Accuracy is important.Billing Provider: Valley Associates, PCNPI: 1476543215Employer ID Number: 16-1234567Address: 1400 West Center Street, Toledo, OH 43601-0213Telephone: 555-967-0303Rendering Provider: Christopher M. Connolly, MDNPI: 8877365552Assignment: AcceptsSignature: On File (01/01/2029)
Ch 15 Case Studies #4
 Prepare the claim for this case by completing the appropriate fields in the CMS-1500 form provided. Accuracy is important. Billing Provider: Valley Associates, PCNPI: 1476543215Employer ID Number: 16-1234567Address: 1400 West Center Street, Toledo, OH 43601-0213Telephone: 555-967-0303Rendering Provider: Christopher M. Connolly, MDNPI: 8877365552Assignment: AcceptsSignature: On File (01/01/2029)
Prepare the claim for this case by completing the appropriate fields in the CMS-1500 form provided. Accuracy is important. Billing Provider: Valley Associates, PCNPI: 1476543215Employer ID Number: 16-1234567Address: 1400 West Center Street, Toledo, OH 43601-0213Telephone: 555-967-0303Rendering Provider: Christopher M. Connolly, MDNPI: 8877365552Assignment: AcceptsSignature: On File (01/01/2029)
Ch 15 Case Studies #5
 Prepare the claim for this case by completing the appropriate fields in the CMS-1500 form provided. Accuracy is important. Billing Provider: Valley Associates, PCNPI: 1476543215Employer ID Number: 16-1234567Address: 1400 West Center Street, Toledo, OH 43601-0213Telephone: 555-967-0303Rendering Provider: Christopher M. Connolly, MDNPI: 8877365552Assignment: AcceptsSignature: On File (01/01/2029)
Prepare the claim for this case by completing the appropriate fields in the CMS-1500 form provided. Accuracy is important. Billing Provider: Valley Associates, PCNPI: 1476543215Employer ID Number: 16-1234567Address: 1400 West Center Street, Toledo, OH 43601-0213Telephone: 555-967-0303Rendering Provider: Christopher M. Connolly, MDNPI: 8877365552Assignment: AcceptsSignature: On File (01/01/2029)
Ch 15 Case Studies #1
 Prepare the claim for this case by completing the appropriate fields in the CMS-1500 form provided. Accuracy is important. Billing Provider: Valley Associates, PCNPI: 1476543215Employer ID Number: 16-1234567Address: 1400 West Center Street, Toledo, OH 43601-0213Telephone: 555-967-0303Rendering Provider: Christopher M. Connolly, MDNPI: 8877365552Assignment: AcceptsSignature: On File (01/01/2029)
Prepare the claim for this case by completing the appropriate fields in the CMS-1500 form provided. Accuracy is important. Billing Provider: Valley Associates, PCNPI: 1476543215Employer ID Number: 16-1234567Address: 1400 West Center Street, Toledo, OH 43601-0213Telephone: 555-967-0303Rendering Provider: Christopher M. Connolly, MDNPI: 8877365552Assignment: AcceptsSignature: On File (01/01/2029)
Ch 8.1 Claim Form
 The objective of these exercises is to correctly complete private payer claims, applying what you have learned in the chapter. Following the information about the provider for the cases are two sections. The first section contains information about the patient, the insurance coverage, and the current medical condition. The second section is an encounter form for Valley Associates, PC. The following provider information should be used for Cases 8.4A and 8.4B Billing Provider Information: Valley Associates, PCAddress: 1400 West Center Street Toledo, OH...
The objective of these exercises is to correctly complete private payer claims, applying what you have learned in the chapter. Following the information about the provider for the cases are two sections. The first section contains information about the patient, the insurance coverage, and the current medical condition. The second section is an encounter form for Valley Associates, PC. The following provider information should be used for Cases 8.4A and 8.4B Billing Provider Information: Valley Associates, PCAddress: 1400 West Center Street Toledo, OH...
Case 7.4 From the Patient Information Form
Provider Information Billing Provider Valley Associates, PC NPI 1476543215Address 1400 West Center Street, Toledo, OH 43601-0213Telephone 555-967-0303Employer ID Number 16-1234567Rendering Provider Christopher M. Connolly, MDNPI 8877365552Oxford PPO Provider Number 1011Oxford HMO Provider Number 2567Assignment AcceptsName Josephine SmithSex FBirthdate 05/04/1994Marital Status MarriedAddress 9 Brook Rd. Alliance, OH 44601-1812Telephone 555-214-3349Employer Central Ohio OilRace WhiteEthnicity Not Hispanic or LatinoPreferred Language EnglishInsured SelfHealth Plan Oxford Freedom HMOInsurance ID Number 610327842XPolicy Number 195803Group Number G0404Copayment/Deductible Amount $10 copayBenefits YSignature on File 01/01/2029Condition Unrelated to Employment, Auto...
Ch 8.2 Claim Form
 The objective of these exercises is to correctly complete private payer claims, applying what you have learned in the chapter. Following the information about the provider for the cases are two sections. The first section contains information about the patient, the insurance coverage, and the current medical condition. The second section is an encounter form for Valley Associates, PC. The following provider information should be used for Cases 8.4A and 8.4B Billing Provider Information: Valley Associates, PCAddress: 1400 West Center Street Toledo, OH...
The objective of these exercises is to correctly complete private payer claims, applying what you have learned in the chapter. Following the information about the provider for the cases are two sections. The first section contains information about the patient, the insurance coverage, and the current medical condition. The second section is an encounter form for Valley Associates, PC. The following provider information should be used for Cases 8.4A and 8.4B Billing Provider Information: Valley Associates, PCAddress: 1400 West Center Street Toledo, OH...
Case 7.3 From the Patient Information Form
Provider Information Billing Provider Valley Associates, PC NPI 1476543215Address 1400 West Center Street, Toledo, OH 43601-0213Telephone 555-967-0303Employer ID Number 16-1234567Rendering Provider Christopher M. Connolly, MDNPI 8877365552Oxford PPO Provider Number 1011Oxford HMO Provider Number 2567Assignment AcceptsInformation About the Patient:Name Kalpesh ShahSex MBirth Date 01/21/2016Marital Status SingleAddress 1433 Third Avenue, Cleveland, OH 44101-1234Telephone 555-608-9772Employer Not EmployedRace WhiteEthnicity Not Hispanic or LatinoPreferred Language English Information About Insured:Name Raj ShahPatient Relationship to Insured ChildSex MBirthdate 02/16/1987Marital Status MarriedAddress 1433 Third Avenue, Cleveland, OH 44101-1234Telephone 555-608-9772Employer Cleveland...
Case 7.2 From the Patient Information Form
In the cases that follow, you play the role of a medical insurance specialist who is preparing HIPAA claims for transmission. Assume that you are working with the practice’s PMP to enter the transactions. The information you enter is based on the patient information form and the encounter form. • Claim control numbers are created by adding the eight-digit date to the patient account number, as in AA026-10042029. • A copayment of $15 is collected from...
Most questions answered within 3 hours.
-
Two blocks of masses m1 and m2 hang at the ends of a string that
passes...
asked 8 seconds from now -
Linear programming is an excellent technique yet is not applied
nearly enough in the “real world.”...
asked 8 minutes ago -
What three alkenes yield 3-methylpentane on catalytic
hydrogenation?
asked 8 minutes ago -
In JAVA Create a program with an array with the following
data:
50 12 31 76...
asked 11 minutes ago -
Using a hormone of the hypothalamic-anterior pituitary axis,
describe or diagram how negative feedback loops regulate...
asked 9 minutes ago -
1,1-dimethylcyclorohexane reacts with single bromine atom
asked 32 minutes ago -
The completed Lewis structure of CO2 contains a total
of 0,1,2,3,4,5,6,7,8 covalent bonds
and 0,1,2,3,4,5,6,7,8 lone pairs.
NOTE:...
asked 39 minutes ago -
A 0.0510 M solution of an organic acid has an
[H+] of 7.50×10-4M .
What is...
asked 36 minutes ago -
what is the profit-maximizing output condition that a
monopolistically competitive firm must satisfy? a) price charged...
asked 40 minutes ago -
Consider the set of ordered pairs shown below. Assuming that the
regression equation is y=3.513+0.429x and...
asked 1 hour ago -
1. (A) Write two
structural (constitutional)
isomers of C4H8F2?
Please show all of
the
asked 1 hour ago -
Objective: Practice converting a Boolean logic
expression into it’s truth table and to show the implementation...
asked 1 hour ago