Ch 8.1 Claim Form
The objective of these exercises is to correctly complete private payer claims, applying what you have learned in the chapter. Following the information about the provider for the cases are two sections. The first section contains information about the patient, the insurance coverage, and the current medical condition. The second section is an encounter form for Valley Associates, PC.
The following provider information should be used for Cases 8.4A and 8.4B
Billing Provider Information: Valley Associates, PC
Address: 1400 West Center Street
Toledo, OH 43601-0213
Telephone: 555-967-0303
Employer ID Number: 16-1234567
NPI: 1476543215
Rendering Provider Information
Name: David Rosenberg, M.D.
NPI: 1288560027
Assignment: Accepts
Signature: On File (01/01/2029)
From the Patient Information Form:
Name: David Belline
Sex: M
Birth Date: 01/22/1968
Marital Status: Married
Address: 250 Milltown Rd.
Alliance, OH
44601-3456
Telephone: 555-627-1535
Employer: Kinko’s
Race: White
Ethnicity: Not Hispanic or Latino
Preferred Language: English
Insured: Self
Health Plan: Anthem BCBS PPO
Insurance ID Number: 35Z29005
Policy Number: 87526
Group Number: 162537B
Copayment/Deductible Amt.: $20 copay
Assignment of Benefits: Y
Signature on File: Y (06/01/2029)
Condition unrelated to Employment, Auto Accident, or Other Accident
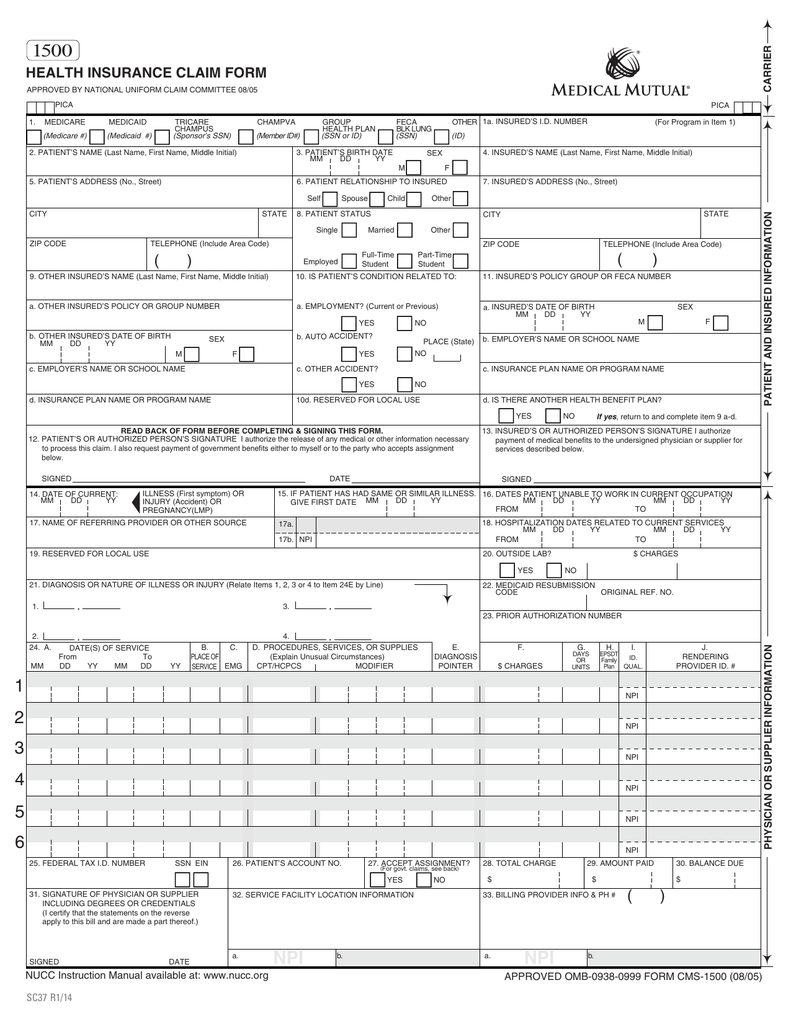
Be sure to follow NUCC directions for CMS-1500 claim completion in regards to punctuation in addresses. Related to this, do not include punctuation for Item Number 31. Follow Medicare guidelines and abbreviate street addresses (i.e. ST rather than Street). Per NUCC Guidelines, use SOF in this exercise for Signature on File if appropriate. Also, per NUCC guidelines, do not include the decimal point in the diagnosis code(s) entered in Item Number 21. Functionality TIP: if you can't see the entire form and don't have scroll bar functionality (especially if you click "Check my work"), click anywhere in the form and use the arrow keys on your keyboard to help you navigate.
![]()
Homework Answers
Request Answer!
11 have requested this problem solution
The more requests, the faster the answer.
Ch 10.1
 The objective of these exercises is to correctly complete Medicaid claims, applying what you have learned in the chapter. Following the information about the provider for the cases are two sections. The first section contains information about the patient, the insurance coverage, and the current medical condition. The second section is an encounter form for Valley Associates, PC. Billing Provider Information Name: Valley Associates, PCAddress: 1400 West Center Street Toledo, OH 43601-0213Telephone: 555-967-0303Employer ID Number: 16-1234567NPI: 1476543215 Rendering Provider Information Name: David Rosenberg, MDNPI: 1288560027Assignment: AcceptsSignature: On File (01/01/2029)
The objective of these exercises is to correctly complete Medicaid claims, applying what you have learned in the chapter. Following the information about the provider for the cases are two sections. The first section contains information about the patient, the insurance coverage, and the current medical condition. The second section is an encounter form for Valley Associates, PC. Billing Provider Information Name: Valley Associates, PCAddress: 1400 West Center Street Toledo, OH 43601-0213Telephone: 555-967-0303Employer ID Number: 16-1234567NPI: 1476543215 Rendering Provider Information Name: David Rosenberg, MDNPI: 1288560027Assignment: AcceptsSignature: On File (01/01/2029)
Ch 8.2 Claim Form
 The objective of these exercises is to correctly complete private payer claims, applying what you have learned in the chapter. Following the information about the provider for the cases are two sections. The first section contains information about the patient, the insurance coverage, and the current medical condition. The second section is an encounter form for Valley Associates, PC. The following provider information should be used for Cases 8.4A and 8.4B Billing Provider Information: Valley Associates, PCAddress: 1400 West Center Street Toledo, OH...
The objective of these exercises is to correctly complete private payer claims, applying what you have learned in the chapter. Following the information about the provider for the cases are two sections. The first section contains information about the patient, the insurance coverage, and the current medical condition. The second section is an encounter form for Valley Associates, PC. The following provider information should be used for Cases 8.4A and 8.4B Billing Provider Information: Valley Associates, PCAddress: 1400 West Center Street Toledo, OH...
Ch 10.2
 The objective of these exercises is to correctly complete Medicaid claims, applying what you have learned in the chapter. Following the information about the provider for the cases are two sections. The first section contains information about the patient, the insurance coverage, and the current medical condition. The second section is an encounter form for Valley Associates, PC. Billing Provider Information Name: Valley Associates, PCAddress: 1400 West Center Street Toledo, OH 43601-0213Telephone: 555-967-0303Employer ID Number: 16-1234567NPI: 1476543215 Rendering Provider Information Name: David Rosenberg, MDNPI: 1288560027Assignment: AcceptsSignature: On File (01/01/2029)nformation About the...
The objective of these exercises is to correctly complete Medicaid claims, applying what you have learned in the chapter. Following the information about the provider for the cases are two sections. The first section contains information about the patient, the insurance coverage, and the current medical condition. The second section is an encounter form for Valley Associates, PC. Billing Provider Information Name: Valley Associates, PCAddress: 1400 West Center Street Toledo, OH 43601-0213Telephone: 555-967-0303Employer ID Number: 16-1234567NPI: 1476543215 Rendering Provider Information Name: David Rosenberg, MDNPI: 1288560027Assignment: AcceptsSignature: On File (01/01/2029)nformation About the...
Ch 15 Case Studies #3
 Prepare the claim for this case by completing the appropriate fields in the CMS-1500 form provided. Accuracy is important.Billing Provider: Valley Associates, PCNPI: 1476543215Employer ID Number: 16-1234567Address: 1400 West Center Street, Toledo, OH 43601-0213Telephone: 555-967-0303Rendering Provider: Christopher M. Connolly, MDNPI: 8877365552Assignment: AcceptsSignature: On File (01/01/2029)
Prepare the claim for this case by completing the appropriate fields in the CMS-1500 form provided. Accuracy is important.Billing Provider: Valley Associates, PCNPI: 1476543215Employer ID Number: 16-1234567Address: 1400 West Center Street, Toledo, OH 43601-0213Telephone: 555-967-0303Rendering Provider: Christopher M. Connolly, MDNPI: 8877365552Assignment: AcceptsSignature: On File (01/01/2029)
Ch 15 Case Studies #4
 Prepare the claim for this case by completing the appropriate fields in the CMS-1500 form provided. Accuracy is important. Billing Provider: Valley Associates, PCNPI: 1476543215Employer ID Number: 16-1234567Address: 1400 West Center Street, Toledo, OH 43601-0213Telephone: 555-967-0303Rendering Provider: Christopher M. Connolly, MDNPI: 8877365552Assignment: AcceptsSignature: On File (01/01/2029)
Prepare the claim for this case by completing the appropriate fields in the CMS-1500 form provided. Accuracy is important. Billing Provider: Valley Associates, PCNPI: 1476543215Employer ID Number: 16-1234567Address: 1400 West Center Street, Toledo, OH 43601-0213Telephone: 555-967-0303Rendering Provider: Christopher M. Connolly, MDNPI: 8877365552Assignment: AcceptsSignature: On File (01/01/2029)
Ch 15 Case Studies #5
 Prepare the claim for this case by completing the appropriate fields in the CMS-1500 form provided. Accuracy is important. Billing Provider: Valley Associates, PCNPI: 1476543215Employer ID Number: 16-1234567Address: 1400 West Center Street, Toledo, OH 43601-0213Telephone: 555-967-0303Rendering Provider: Christopher M. Connolly, MDNPI: 8877365552Assignment: AcceptsSignature: On File (01/01/2029)
Prepare the claim for this case by completing the appropriate fields in the CMS-1500 form provided. Accuracy is important. Billing Provider: Valley Associates, PCNPI: 1476543215Employer ID Number: 16-1234567Address: 1400 West Center Street, Toledo, OH 43601-0213Telephone: 555-967-0303Rendering Provider: Christopher M. Connolly, MDNPI: 8877365552Assignment: AcceptsSignature: On File (01/01/2029)
Ch 15 Case Studies #1
 Prepare the claim for this case by completing the appropriate fields in the CMS-1500 form provided. Accuracy is important. Billing Provider: Valley Associates, PCNPI: 1476543215Employer ID Number: 16-1234567Address: 1400 West Center Street, Toledo, OH 43601-0213Telephone: 555-967-0303Rendering Provider: Christopher M. Connolly, MDNPI: 8877365552Assignment: AcceptsSignature: On File (01/01/2029)
Prepare the claim for this case by completing the appropriate fields in the CMS-1500 form provided. Accuracy is important. Billing Provider: Valley Associates, PCNPI: 1476543215Employer ID Number: 16-1234567Address: 1400 West Center Street, Toledo, OH 43601-0213Telephone: 555-967-0303Rendering Provider: Christopher M. Connolly, MDNPI: 8877365552Assignment: AcceptsSignature: On File (01/01/2029)
Case 7.4 From the Patient Information Form
Provider Information Billing Provider Valley Associates, PC NPI 1476543215Address 1400 West Center Street, Toledo, OH 43601-0213Telephone 555-967-0303Employer ID Number 16-1234567Rendering Provider Christopher M. Connolly, MDNPI 8877365552Oxford PPO Provider Number 1011Oxford HMO Provider Number 2567Assignment AcceptsName Josephine SmithSex FBirthdate 05/04/1994Marital Status MarriedAddress 9 Brook Rd. Alliance, OH 44601-1812Telephone 555-214-3349Employer Central Ohio OilRace WhiteEthnicity Not Hispanic or LatinoPreferred Language EnglishInsured SelfHealth Plan Oxford Freedom HMOInsurance ID Number 610327842XPolicy Number 195803Group Number G0404Copayment/Deductible Amount $10 copayBenefits YSignature on File 01/01/2029Condition Unrelated to Employment, Auto...
Case 7.3 From the Patient Information Form
Provider Information Billing Provider Valley Associates, PC NPI 1476543215Address 1400 West Center Street, Toledo, OH 43601-0213Telephone 555-967-0303Employer ID Number 16-1234567Rendering Provider Christopher M. Connolly, MDNPI 8877365552Oxford PPO Provider Number 1011Oxford HMO Provider Number 2567Assignment AcceptsInformation About the Patient:Name Kalpesh ShahSex MBirth Date 01/21/2016Marital Status SingleAddress 1433 Third Avenue, Cleveland, OH 44101-1234Telephone 555-608-9772Employer Not EmployedRace WhiteEthnicity Not Hispanic or LatinoPreferred Language English Information About Insured:Name Raj ShahPatient Relationship to Insured ChildSex MBirthdate 02/16/1987Marital Status MarriedAddress 1433 Third Avenue, Cleveland, OH 44101-1234Telephone 555-608-9772Employer Cleveland...
Case 7.2 From the Patient Information Form
In the cases that follow, you play the role of a medical insurance specialist who is preparing HIPAA claims for transmission. Assume that you are working with the practice’s PMP to enter the transactions. The information you enter is based on the patient information form and the encounter form. • Claim control numbers are created by adding the eight-digit date to the patient account number, as in AA026-10042029. • A copayment of $15 is collected from...
Most questions answered within 3 hours.
-
Little’s Law: Val d’Costa is a world famous ski village in the
French Alps. Because of...
asked 25 minutes ago -
Find the absolute error D for the calculation if A + B/C=D A=
9.4 +/- 0.4...
asked 38 minutes ago -
New Air Heating and Cooling, manufactures furnaces and central
air units. The company pride itself on...
asked 52 minutes ago -
A coach uses a new technique to train gymnasts. Seven
gymnasts were randomly selected and their...
asked 2 hours ago -
While rotating the tires on your car you notice a rock [mass =
0.1 Kg] stuck...
asked 4 hours ago -
Using MARS simulator, write MIPS programs according to
the following scenarios: Receive a positive integer number...
asked 6 hours ago -
An object in front of a concave mirror has a real image that is
11.5 cm...
asked 6 hours ago -
Consider the reaction, C3 H8 + O2 --> CO2 + H2O. How many
moles of O2...
asked 8 hours ago -
You and your opponent both roll a fair die. If you both roll the
same number,...
asked 8 hours ago -
In a study of the accuracy of fast food drive-through orders,
Restaurant A had 257 accurate...
asked 8 hours ago -
Identify and describe in detail the four categories of
institutions that could be included in a...
asked 9 hours ago -
In python
class Customer:
def __init__(self, customer_id, last_name, first_name, phone_number, address):
self._customer_id = int(customer_id)
self._last_name =...
asked 9 hours ago